Summary
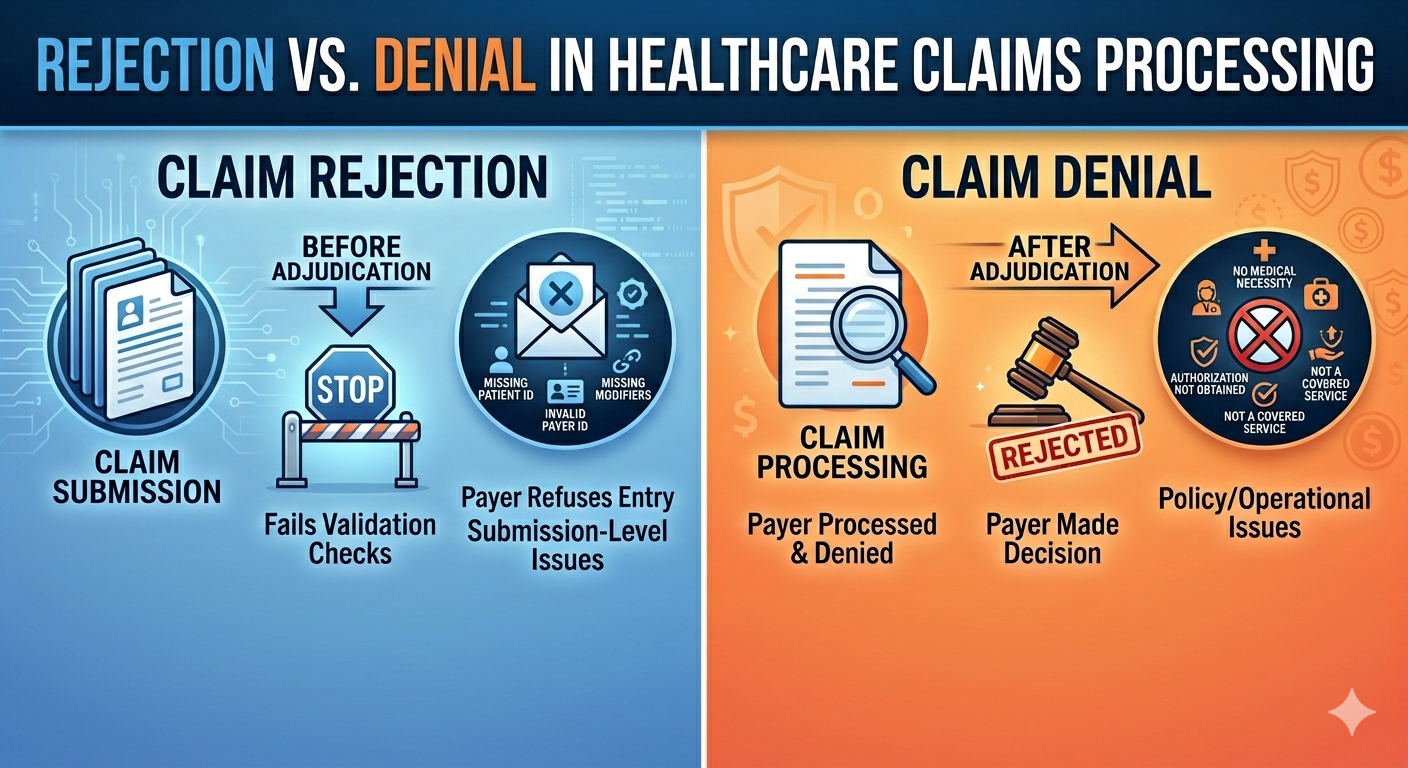
The difference between rejection vs denial is one of the most misunderstood concepts in healthcare revenue cycle management. While both delay reimbursement, they occur at different stages of claims processing and require completely different operational responses. Rejections occur before the payer processes the claim, usually because of submission errors or missing data. Denials occur after adjudication when the payer determines the claim does not meet reimbursement requirements. Healthcare organizations that fail to distinguish between the two often experience recurring cash flow problems, increased administrative burden, preventable revenue leakage, and long-term operational inefficiencies.
Why Understanding the Difference Matters More Than Most Practices Realize
A healthcare practice can provide excellent clinical care, maintain strong patient relationships, and still struggle financially because of one simple issue: the practice does not fully understand the difference between a claim rejection and a claim denial.
To many providers and even some billing teams, the two terms sound interchangeable. They are often used casually in conversations as if they represent the same operational problem. They do not. And misunderstanding that distinction can create delays in cash flow, increased accounts receivable, staff inefficiency, compliance exposure, and long-term revenue instability.
The reality is this: a rejected claim and a denied claim occur at two completely different stages of the revenue system.
One typically represents a failure before the claim even enters the payer adjudication process. The other represents a failure after the payer has already reviewed the claim.
Understanding where the failure occurred is critical because it determines who should fix the issue, how the issue should be corrected, how quickly revenue can be recovered, and whether the underlying problem is operational or structural.
Practices that fail to understand this distinction often spend excessive time “working denials” that were never true denials in the first place, while simultaneously overlooking the upstream operational failures causing the problems repeatedly.
In many cases, rejection and denial patterns are not merely billing problems. They are signals of deeper revenue system fractures.
What Is a Claim Rejection?
A claim rejection occurs when a claim fails validation checks before the payer formally processes or adjudicates the claim.
In simpler terms, the claim is returned because something is wrong with the submission itself. The payer or clearinghouse refuses to accept the claim into processing. The claim essentially fails the “entry requirements” needed to move into adjudication.
Common reasons for claim rejections include:
- Missing patient information
- Incorrect subscriber ID numbers
- Invalid payer ID selection
- Missing modifiers
- Invalid diagnosis or procedure code formatting
- Incorrect provider identifiers
- Demographic mismatches
- Claims submitted to the wrong payer
- Missing authorization information
- Incomplete claim fields
A rejection is often considered a front-end or submission-level problem.
The important distinction is this: the payer usually has not yet made a payment decision. The claim never successfully entered the adjudication workflow.
What Is a Claim Denial?
A denial occurs after the payer receives, reviews, and adjudicates the claim but decides not to pay all or part of it.
Unlike a rejection, the claim successfully entered the payer’s processing system. The payer reviewed the claim and made a determination.
That determination may involve:
- No payment
- Reduced payment
- Requests for additional information
- Determination that the service is not payable under the policy terms
Common denial reasons include:
- Medical necessity issues
- Authorization not obtained
- Timely filing exceeded
- Non-covered services
- Coordination of benefits issues
- Credentialing or contracting problems
- Documentation deficiencies
- Duplicate claims
- Frequency limitations
- Eligibility termination
- Incorrect place of service
- Bundling edits
- Policy exclusions
A denial is therefore not simply a data-entry problem. It is often a policy, documentation, operational, contractual, or clinical validation issue.
Why the Difference Matters
Many healthcare organizations incorrectly group rejections and denials together under the broad category of “billing issues.” That creates operational blind spots.
Rejections and denials often point to failures occurring in entirely different layers of the revenue system.
For example:
| Issue Type | Common Revenue System Layer |
| Rejections | Capture Layer |
| Denials | Collection or Protection Layer |
A rejection often indicates poor intake workflows, weak eligibility verification, incorrect payer setup, coding submission errors, or a lack of process standardization.
A denial may indicate authorization failures, documentation weaknesses, poor payer policy management, credentialing issues, inadequate clinical validation, or contract misalignment.
The operational response should therefore be different. Treating both the same leads to repetitive failures.
The Financial Impact of Rejections
Many practices underestimate the damage caused by rejections because they assume rejected claims are “easy fixes.” That assumption is dangerous.
Even small rejection percentages can create delayed revenue, increased staff labor, resubmission bottlenecks, delayed patient statements, aging accounts receivable, and cash flow instability.
The problem compounds because rejected claims often sit untouched in work queues for days or weeks before correction. During that time, filing deadlines continue, patient balances remain unresolved, and reimbursement delays expand.
A practice processing 3,000 claims monthly with even a 5 percent rejection rate may be dealing with 150 operational interruptions every single month.
That is not a small issue. That is a structural performance problem.
The Financial Impact of Denials
Denials are typically more expensive than rejections because the claim has already entered adjudication and failed after review.
Denials frequently require appeals, medical records, payer calls, corrected claim submissions, reconsiderations, or provider involvement.
Denials also consume substantially more labor hours.
In many organizations, denial management becomes reactive instead of strategic. Teams become trapped in endless recovery activity instead of fixing the underlying causes.
This creates a dangerous operational cycle:
- Claims denied
- Staff work denials
- Revenue delayed
- Teams overwhelmed
- Root causes ignored
- Same denials repeat
Over time, this erodes both operational efficiency and financial predictability.
Rejections and Denials Are Often Symptoms, Not Root Causes
One of the biggest mistakes healthcare practices make is treating rejection and denial management as isolated billing tasks.
In reality, these issues are frequently downstream manifestations of upstream operational failures.
A denial for authorization may actually originate from poor scheduling workflows, inadequate intake communication, or unclear staff accountability.
A rejection for subscriber mismatch may originate from rushed registration processes, lack of front-desk training, or absence of verification protocols.
This is why practices that focus only on “working denials harder” often fail to improve overall financial performance.
You cannot permanently solve revenue problems downstream if the upstream system remains broken.
The Difference Between Operational Errors and Structural Problems
Not every rejection or denial indicates a broken system. Some are isolated operational errors.
However, patterns matter.
If the same rejection or denial types occur repeatedly, the practice likely has a structural revenue system problem.
Examples of structural issues include:
- Inconsistent workflows
- Lack of accountability
- Missing policies
- Insufficient training
- Fragmented communication
- Poor payer management
- Weak governance
- Absence of standardized procedures
At that point, the issue is no longer about one claim. The issue is about the system itself.
How Strong Practices Reduce Rejections and Denials
High-performing healthcare organizations do not merely “work claims.” They build revenue protection systems.
That includes:
- Standardized intake workflows
- Strong benefit verification processes
- Authorization tracking systems
- Payer policy monitoring
- Credentialing oversight
- Quality assurance reviews
- Denial trend analysis
- Staff accountability structures
- Continuous operational audits
More importantly, strong organizations understand that revenue performance is not solely determined by billing activity. Revenue performance is determined by how well the entire operational system functions together.
Key Questions Every Practice Should Ask
Healthcare organizations should regularly evaluate:
- What are our top rejection reasons?
- What are our top denial reasons?
- Are patterns increasing or decreasing?
- Which departments contribute most to failures?
- Are the issues operational or structural?
- How much labor is spent on rework?
- How much revenue is delayed monthly?
- What percentage of denials are preventable?
- Are workflows standardized?
- Are staff properly trained and accountable?
Without these answers, practices often operate reactively instead of strategically.
Key Takeaways
- Rejections occur before adjudication; denials occur after adjudication.
- Rejections are usually submission-level issues.
- Denials often involve documentation, authorization, or payer policy issues.
- Both can significantly delay revenue and increase administrative costs.
- Repeated patterns often signal structural operational weaknesses.
- Strong healthcare organizations focus on prevention, not just rework.
- Revenue cycle performance depends on operational alignment across departments.
Conclusion
A rejection is not the same as a denial. And misunderstanding that difference can quietly damage an organization’s financial performance for years.
Rejections often indicate failures before adjudication. Denials often indicate failures after adjudication.
Both matter. But more importantly, both are signals. Signals that reveal how well — or how poorly — the revenue system is functioning.
Practices that merely process claims will continue fighting recurring operational fires. Practices that understand the deeper structure of the revenue system can identify problems earlier, reduce preventable revenue leakage, improve operational performance, and create greater long-term financial stability.
Because in healthcare, financial performance is rarely determined by one isolated billing issue. It is determined by the strength of the system behind it.
A Final Consideration
If your organization is experiencing recurring rejections, increasing denial rates, delayed collections, or ongoing revenue instability, the issue may not simply be billing activity alone. In many cases, these patterns are indicators of deeper operational or structural weaknesses within the broader revenue system.
Sometimes, the most valuable step is not immediately changing staff or software, but first gaining clarity on where the actual breakdowns exist.
At L&C Advanced Practice Management, we work with healthcare organizations to evaluate the broader operational and financial systems that impact revenue performance, including front-end workflows, payer processes, revenue protection strategies, credentialing structures, and claims performance trends.
For organizations looking to better understand where revenue problems may be originating, a Revenue Diagnostic can often provide meaningful insight into both operational inefficiencies and structural revenue gaps.
Revenue Diagnostic:
Schedule a Diagnostic Call
Educational Insights and Revenue Strategy Discussions:
Christopher Bass YouTube Channel
Frequently Asked Questions: Rejection vs. Denial in Healthcare Claims Processing
A rejection occurs before the payer processes the claim because of submission or formatting errors. A denial occurs after the payer reviews the claim and determines payment should not be issued fully or partially.
Denials are generally more expensive because they often require appeals, payer communication, and additional documentation. However, high rejection rates can also create major operational inefficiencies and delayed cash flow.
L&C Advanced Practice Management helps healthcare organizations evaluate operational and structural revenue cycle weaknesses that contribute to recurring denials, rejections, delayed reimbursements, and cash flow instability. Their Revenue Diagnostic process focuses on identifying workflow inefficiencies, payer process gaps, credentialing issues, authorization failures, and revenue protection opportunities across the healthcare revenue cycle.